This review, after a quick overview of the evolution of Italian legislation on driving tests, proposes an in-depth examination of the visual parameters that the most recent legislation has identified as necessary requirements for the issue and renewal of driving licences.
During these years, the characteristics, potential and danger of motor vehicles have changed considerably. Likewise, there has been an evolution of the basic requirements for obtaining and renewing a driving licence.
I visual requirements are becoming increasingly predominant, in fact, according to Hills1 the 90% of the information needed to drive a motor vehicle is visual.
Safety on the road, therefore, depends not only on a driver's psychological fitness, behavioural habits and reaction time, but is also closely linked to visual function2-5. The importance of the visual apparatus is also underlined by the analysis of Istat data on the distribution of accidents throughout the day6.
Please refer to Annex A of the legislative decree for the modalities of the tests and the necessary visual requirements No. 59 of 18 April 2011implementing Directives 2006/126/EC and 2009/113/EC, published in Official Gazette No. 99 of 30-4-2011 and Table 1.
 Visual acuity
Visual acuity
Defined as the eye's ability to resolve and perceive fine details of an object, it depends directly on the sharpness of the image projected onto the retina8.
It is measured using the best visual correction using a classical optotype and is reported in tenths.
In case of ametropiathe simplest correction is entrusted to the glassesThey must be of good quality, non-coloured except in the case of sunglasses and provided with effective UV shielding (especially UV-B), although contact lenses (L.A.C.) are increasingly used lately, especially in younger and more dynamic patients. Spectacles do not offer perfect corrections for the high ametropias, encounter difficulties in correcting anisometropies (high differences between the two eyes), reduced field of vision, not always perfect three-dimensionality, lens fit problems (Figure 1).
Le LAC offer potentially perfect and very 'natural' correction with an extended visual field, although they require careful maintenance, are a risk factor for keratitis and are not well tolerated especially by patients suffering from allergies and dry eye9-10.
Field of vision
Another prerequisite is the assessment of the extension of the bilateral visual field: when driving a vehicle, but also for pedestrians in traffic, having a static and dynamic visual field of 'normal' extension is absolutely essential (Figure 2).
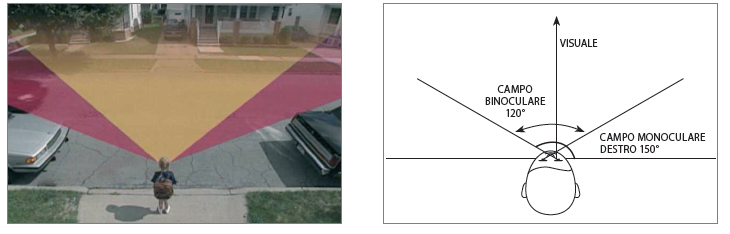
In fact, as mentioned earlier most accidents occur in traffic and an intact field of vision allows us to detect a lateral danger without taking our eyes off the fixation point9.
Contrast sensitivity
Contrast sensitivity is a measure of the minimum amount of contrast required to recognise an object under examination. The test can identify very early visual dysfunctions, even when visual acuity is normal with the Snellen test.
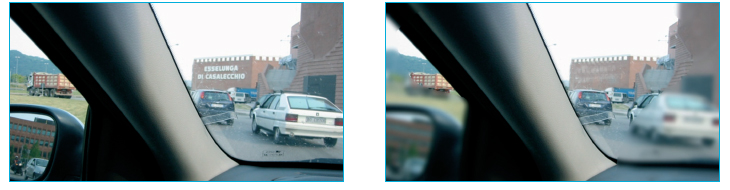
It is a function of the visual apparatus of primary importance in everyday life and especially behind the wheel. Although many stimulations during driving involve high-contrast objects (road signs), weather or environmental conditions and the dulling of the windscreen as a result of the accumulation of debris, insects and moisture can drastically reduce image contrast (Figure 3). Therefore, contrast sensitivity has proven to be a very sensitive indicator of visual performance when driving a motor vehicle.9-13.

Recently, the effect of reduced contrast sensitivity was documented by simulating a salt water film on the car windscreen14. Under these conditions, which are very frequent in our latitudes during winter periods, the additive effect of an intrinsic deficit in contrast sensitivity can be potentially very dangerous, especially if the driver in question is elderly and shows a slowdown in reaction time.
The ability to distinguish stationary or transient stimuli with a low luminance or reflectance difference to the surrounding environment is, therefore, a fundamental requirement for driving skills.
Ifnsitivity to glare
Glare sensitivity is defined as the ability to see after being dazzled. At the side of the monitor are two high beam lights oriented towards the subject to be examined to simulate the headlights of a frontal car. The light forms an angle of 30 degrees to the subject. The headlights emit a very bright light for 60 seconds during which the subject is asked to read and recognise the letters. While driving, it is not difficult to be dazzled by sunlight reflecting off a flat surface (water, snow, wet road surface, windscreen) which creates annoying reflections, altering the perception of shapes, colours and contrasts.
Glare, traditionally distinguished into glare with discomfort (discomforting glarethe severity of which is difficult to quantify) and glare with reduced performance visual, can be aggravated by factors such as opacification of the dioptric media (particularly cataracts) and subsequent intraocular lens implantation15,16 and advanced age in general9,10,17,18.
It is well known that people with cataracts (figure 4) not only experience reduced visual acuity, reduced contrast, but also report discomfort when driving at night due to the presence of light halos around headlights.
The techniques are based on a comparison of the measurement of the recognition threshold in the absence and in the presence of a dazzling light source (whereby the susceptibility to glare is proportional to the magnitude of this discrepancy) and differ in the characteristics of the targetof the dazzling light source and for the luminance values adopted ?
Recovery time after glare
This value expresses the time required to recover sufficient vision after being dazzled. One eye at a time is dazzled very closely through a light source for ten seconds, the light source is removed, the letters are presented to the monitor and asked to recognise them.
This is a crucial aspect in judging fitness to drive as there are many sources of glare while driving a vehicle: think of the headlights of other cars or when exiting a tunnel9. A prolonged glare recovery time is therefore a danger. ".
Recovery time after glare is known to increase with age9,19,20. Schieber20, for example, showed that this latency for low-contrast supra-threshold stimuli in an older group of subjects (age: 65-74 years) was three times higher than in a younger sample (age: 18-24 years) (2142 msec. vs. 790 msec.). It should be emphasised that this increase occurred despite the fact that in the older group the contrast levels of the stimuli to be recognised had been increased by 0.1 logarithmic units above the level adopted for the other group, in order to prevent the well-known reduction in contrast sensitivity with age from influencing the result. The authors conclude that after glare older drivers lose visual contact with low-contrast stimuli for more than 2 seconds.

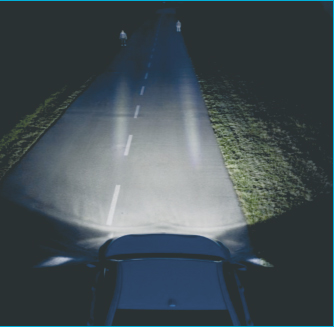
Twilight vision
Dark adaptation is the phenomenon whereby the visual system (pupil, retina and occipital cortex) adapts to reduced brightness. It is performed in a darkened room, the monitor screen is also dark, and letters are asked to be recognised. It is easy to see that this visual function is of paramount importance in order to be able to detect pedestrians, stopped vehicles or other obstacles and to have sufficient time to stop or deviate (figure 5).

The consequences of a deficit in contrast sensitivity can be aggravated not only by an increased susceptibility to glare, but also by conditions of poor lighting. In this regard, it is established that in many rural roads with poor lighting, the resulting environmental contrast values are among those often found to be deficient in the older population20.
To these environmental and physiological aspects that cannot be changed much more, pathological conditions can be added that further reduce visual capacity in crepuscular or scotopic conditions, such as cataracts or, more rarely, retinosis pigmentosa. Cataract patients in particular may demonstrate a significant discrepancy between visual acuity in the dark or in sunlight21while it is even pathognomonic of retinosis pigmentosa to have poor sensitivity to darkness, which is associated in the advanced stages of the disease with a very severe contraction of the visual field.
Considering these special aspects in the requirements for fitness to drive in the latest regulations, the examining board may declare the person fit for daytime driving only.
Interactions between visual parameters
After analysing the rationale of each visual requirement individually, it is easy to see how these functions are not independent of each other, but rather influence each other. An example of this is provided by Bachman14. The result of a loss of contrast can be greatly enhanced by the sun-induced glare effect or the sudden appearance of a light source directed towards the driver, resulting in a major diffraction phenomenon; this loss of contrast can also be worsened by a slow recovery after glare.
To understand the importance of the above-mentioned psychophysical requirements even better, let us give the following example: a driver is driving a car at 100 km/h and suddenly perceives a danger, considering that the reaction time is between 7-10 tenths of a second, the driver makes about 20 metres before putting his foot on the brake. The braking distance, which varies depending on the efficiency of the vehicle, averages about 40 metres. So the car in question will stop about 60 metres after the perception of danger. If the visual system, however, does not allow us to instantly perceive the danger for every additional second the car will have travelled about 27.8 metres: the length of about three lorries, an infinite space.
Conclusions
Road safety depends overwhelmingly on efficient visual performance, which explains the recent regulatory focus on visual requirements for fitness to drive
In addition, it must be emphasised that the new directive in force stipulates that the certificate of newly introduced examinations can be reported by the ophthalmic specialist not only from public facilities.
A few observations arise at this point:
- Do the monocratic doctors have the appropriate equipment to perform them?
- Have the ASLs adapted to current regulations?
- Will these tests actually be performed by the candidates?
- And, finally, what should be the fair cost of the 'licence renewal package', since it is not difficult to surf the Internet and find offers for a few tens of euros?
If one considers that 59.13% of road accidents are directly or indirectly attributable to impairments in visual functions, then one can well understand that these questions are entirely legitimate in order to protect one's own safety and that of others.
Prof. Nicola Pescosolido
Department of Cardiovascular, Respiratory, Nephrological and Geriatric Sciences'.
Faculty of Medicine and Dentistry
Sapienza' University of Rome
Dr Francesco Parisi
Sense Organs Department
Faculty of Medicine and Dentistry
Sapienza' University of Rome
Bibliography'.
1. Hills BL. Vision, visibility, and perception in driving. Perception 1980;9:183-216.
2. Johnson CA, Keltner JL. Incidence of visual field loss in 20000 eyes and its relationship to driving performance. Arch Ophthalmol 1983;101:371-375.
3. Davison PA. Inter-relationships between British drivers' visual abilities, age and road accident histories. Ophthalmic Physiol Opt 1985;5:195-204.
4. Charman WN.Visual standards for driving. Ophthalmic Physiological Optics 1985;5: 211-220.".
5. Marron JA, Bailey IL. Visual factors and orientation and mobility performance. Am J Optom Physiol Opt 1982;59: 413-426.
6. Istat/ACI Report - Road accidents year 2007, Rome, 2008.
7. Maffioletti S., Pocaterra R., Tavazzi S. The importance of correct visual compensation for safe driving. University of Milan Bicocca. Degree course in Optics and Optometry. January 2009.
8. Cline D., Hofstetter H.W., Griffin J.R., Dictionary of Visual Science, 4th edition, Boston, Butterworth-Heinemann, 1996, pp. 820.
9. Pescosolido N. Automotive driving and visual efficiency. Fabiano editore 2001, pp. 127-198.
10. Pescosolido N. Low vision. Visual rehabilitation in automobile driving. Fabiano publisher 2002.
National Research Council. U.S. Committee on Emergent Techniques for Assessment of Visual Parameters. National Academy Press, 1985,Washington, DC.
12. Bachman WG, Egenmaire W. Assessment of cycloplegic effects on the vistech contrast sensitivity test in Army aviator candidates. Optom Vis Sci 1991; 68: 452-455.
13. Bachman WG, Behar I. The effect of cycloplegia on the visual contrast sensitivity function. Aviat Space Environ Med 1987;58: 339-342.
14. Bachman WG, Wingert TA, Bassi CJ. Driver contrast sensitivity and reaction times as measured through a salt-covered windshield. Optometry 2006;77: 67-70.
15. Coupland SG, Kirkham TH. Improved contrast sensitivity with antireflective coated lenses in the presence of glare. Can J Ophthalmol 1981;16: 136-140.
16. Nadler DJ, Jaffe NS, Clayman HM, Jaffe MS, Luscombe SM. Glare disability in eyes with intraocular lenses. Am J Ophthalmol 1984;97: 43-47.
17. Wolf E. Glare and age. Arch Ophthalmol 1960;64: 502-514.
18. Zeimer RC, Noth JM. A new method of measuring in vivo the lens transmittance, and study of lens scatter, fluorescence and transmittance. Ophthalmic Res 1984;16: 246-255.
19. Olson PL, Sivak M. Glare from automobile rear-vision mirrors. Human Factors 1984;26:269-282.
20. Schieber F, Kline DW, Kline TJB, Fozard JL. Contrast sensitivity and the visual problems of older drivers. Society of Automotive Engineers, SAE Technical Paper No. 920613, 1992, Warrendale, PA.
21. Abrahamsson M, Sjostrond J. Impairment of Contrast Sensitivity Function (CSF) as a Measure of Disability Glare. Invest Ophthalmol Vis Sci 1986;27: 1131- 1136.
Dr. Carmelo Chines
Direttore responsabile