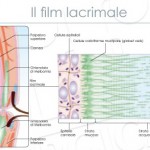
Dry eye is among the most frequent pathological conditions in ophthalmology. Up to 20% of adults over the age of 40 have dry eye symptoms. The origin of this disease is believed to be multifactorial and related to pathological conditions of one of the portions of the functional unit that includes the tear film, the ocular surface (cornea, conjunctiva, accessory lacrimal glands, meibomian glands, the mucus-epidermal junction, a main lacrimal gland and nerve connection systems, excretory ducts and the naso- lacrimal sac.
In the presence of dry eye conditions, both the lachrymal film and the conjunctival horny epithelia undergo important changes that, when chronic, are capable of developing phenomena similar to those present during inflammation on the ocular surface.
Indeed, a tear instability or altered tear composition is associated with an increase in the osmolarity of the aqueous layer of the tear film due to excessive evaporation and increased electrolyte concentration.
A condition of hyper-osmolarity not only causes damage through direct toxicity on the epithelial cell membrane, but also triggers an inflammatory response and stimulates the activation of metallo proteinases on the ocular surface, thus establishing a worsening vicious circle that maintains and extends the damage.
An inflammatory phenomenon, linked to the presence of factors arising from the arachidonic acid cascade, related to hyperosmolar damage to the epithelial membrane, is therefore easy to establish in a dry eye. If this inflammatory condition tends towards chronicity, in predisposed individuals, immune-mediated inflammation may set in.
Inflammation thus becomes one of the central points of the vicious circles tending towards self-maintenance that underlie the formation and maintenance of dry eye damage.
1) If you see a red eye, think 'dry eye'.
2) Consider all concomitant pathologies
3) Break as many vicious circles as possible
If one wants to be effective in the therapeutic approach to this disease, it is essential to bear in mind certain fundamental concepts that are intrinsic to the conception of the ocular surface as a functional unit. Mainly, it is useful to consider that a stable tear film is the result of the harmonisation of a series of complex systems, that a good tear function requires the integrity of the anatomy and epithelial structure, but also an efficient sensory innervation and a good motor function of the apparatuses composing the surface itself.
It is evident at this point that a therapy for dry eye will have to adequately consider all the various components involved and if possible correct those that are inefficient.
It follows from this that a therapy for dry eye symptoms cannot only be directed at restoring tear volume, but must address the different mechanisms involved in the pathogenesis of the damage in the different localisations.
The effects and causes of poor tear production, reduced tear clearance, tear film instability, the presence of a disease of the Meibomian glands and the consequent hyper-evaporation, a deficiency of mucipar cells or reduced secretion of mucins by the epithelia, with the consequent poor lubrication, the presence of epithelial damage and poor blinking habits with the consequent problems of tear distribution, must therefore be addressed.
The therapeutic options for dry eye include the possibility of replacing (at least in volume) the missing tears, the possibility of preserving the tears present, the possibility of stimulating the production of tears or at least certain components and finally the possibility of reducing the inflammatory state always associated with dry eye.
Stimulation of tear production would appear to be possible by administering systemic drugs such as bromhexine, pilocarpine and cevimelin. The results of this systemic stimulation of tear secretion are, however, modest and often do not affect the complaints complained of by patients.
The cornerstones of therapy aimed at increasing the tear volume available to the ocular surface are mainly tear substitutes.
They have an essentially palliative purpose, i.e. aimed at reducing symptoms and partially reducing signs, without however achieving any real curative activity.
These products aim to achieve good lubrication of the interface between the eyelids and the eyeball, create a protective film in front of the epithelium and dilute the contents of the tear film. In particular, they modify the concentration of the electrolytes contained in the film, which are responsible for the hyper-osmolar shift in the tear film, which is typical of dry eye forms and one of the main causes of damage.
The tear substitutes available are mainly eye drops, in multi-dose and single-dose formulations, and gels also in multi-dose and single-dose formulations. Ointments are mainly used during the night, in more advanced forms.
Water-soluble inserts, although useful, were only for limited numbers of patients and have practically disappeared from the market.
In addition to water, tear substitutes consist of polymers, which serve to disperse it evenly and retain it on the surface of the eye.
The most classic formulations, which appeared as early as the early 1970s, use cellulose ethers such as methyl cellulose, hydroxypropyl methyl cellulose and hydroxymethyl cellulose. These preparations exhibit a viscosity that is strictly dependent on the concentration of the principle, and therefore, for reasons mainly of optics and comfort in general, it is not possible to increase the viscosity above well-defined limits. An 1% preparation is in fact one that may be, even if acceptable, uncomfortable for visual function. Most preparations in fact have concentrations around 0.3-0.5%.
The ability to retain water, typical of cellulose derivatives, is also present in preparations based on povidone, polyvinylalcohol, polyethylene glycol, which are thus able to increase the presence of water on the ocular surface and improve lubrication, simply in relation to the amount of water they are able to retain.
Emerging in the mid-1980s, hyaluronic acid derivatives present an important activity capable of beneficially influencing lubrication. In fact, these preparations show a true viscoelastic activity linked to their non-newtonian characteristics. In fact, they have the ability to modify their viscosity depending on the rubbing speed to which they are subjected. In other words, when the eye is open, the viscosity of the tear substitute is high and thus a stable film is formed on the surface of the eye, but during blinking the viscosity rapidly drops. In this way, the blinking is unnoticed and the product very well accepted by the patient.
Of importance is the need to avoid the occurrence of chronic preservative toxicity in these patients in whom, due to high evaporation and low fluid production, tear turnover is reduced. This is followed by an increase in the concentration of the preservative present in the administered eye drops with the associated toxic risks, which are sometimes very significant.
In general, with all the necessary caveats, it is considered that if a tear substitute has to be instilled four or more times a day, it is highly recommended to use a preservative-free formulation.
More recently, lipid-based or lipid-containing tear substitutes have been investigated that should replace or supplement existing ones, improving film stability and reducing evaporation. Apparently, preliminary results look very promising.
Studies aimed at characterising the different cellular and biochemical reactive components that accompany the presence of lacrimal alterations at the ocular surface have highlighted the presence of factors, markers and activators typical of inflammatory forms in the course of these diseases.
Typical increases in interleukins, adhesion molecules and markers of immune activation led to dry eye being considered an inflammatory disease even in the absence of the typical clinical signs of pain, redness, heat, oedema and loss of function.
Clinical studies have shown that the use of corticosteroids in preservative-free eye drops can rapidly improve symptoms, but also the epithelial anatomical picture of patients with dry eye.
The recent commercialisation in the USA of Cyclosporin A in 0.05% eye drops has confirmed the possibility of improving tear performance by reducing the inflammatory state. However, clinical data show that more than one month of continuous treatment (often two) is required to exert a noticeable effect on the patient. Given the cost of the preparation, patients, disheartened by the lack of results, often discontinue treatment before the effectiveness of the therapy can be verified.
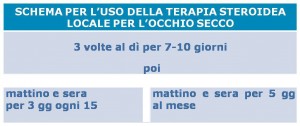
A local steroid treatment, on the other hand, is able to give results very quickly and can be used in the early stages to overcome the delayed activity of Cyclosporin A.
Since prolonged continuous therapy is known to be associated with major eye complications, therapy with non-preserved topical steroids can be used in a pulsed fashion with good results. In this way, by minimising the risks of hypertonus and cataracts, it is possible to maintain the calmness of the ocular surface over time, also making artificial tear replacement therapy more effective.
Try it out,
Prof. Maurizio Rolando
Department of Neuroscience, Ophthalmology and Genetics
University of Genoa
Dr. Carmelo Chines
Direttore responsabile