Ruptured ocular capillaries are a fairly frequent occurrence that often resolve without treatment, but can be an indicator of more important pathologies.
Patient selection for cataract surgery with toric IOLs is a very delicate subject and José L. Güell is a particularly suitable interlocutor to discuss it.
José L. Güell, in fact, is not only among the best refractive cataract surgeons, but also has an all-round scientific background as professor of Ophthalmology and coordinator of ESASO courses. Furthermore, he is known in the international scientific environment as past-president of EUCORNEA and ESCRS.
Fig. 1. Pre-operative markers.
What is the ideal patient for refractive cataract surgery with a toric IOL? The accuracy of astigmatism correction with most currently available pseudophakic toric IOLs is very high.
The majority of models have shown great predictability and, more importantly, stability of correction.
This is the reason why today, in my clinical practice, most patients with stable corneal astigmatism are considered good candidates for the implantation of a toric IOL.
Taking into account the assured rotational stability of most IOL models, the critical point is proper alignment. Therefore, an appropriate pre-operative assessment, including both anterior and posterior corneal astigmatism, as well as a suitable surgical alignment technique are absolutely essential.
Fig. 2. Pre-operative marking at the ophthalmoscope.
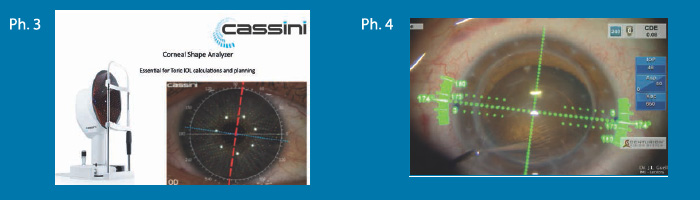
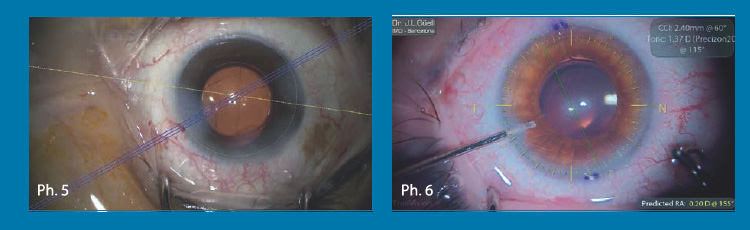
Of the alignment techniques currently available, we can use the simpler ones or the more sophisticated ones, without significant clinical and refractive differences between them, if we review the published works. On the side of the simpler techniques, I would like to mention the use of a pre-operative reference mark (on the ophthalmometer or with the Elies marker or the Robomarker, for example) or the use of the topographic image on a high quality photograph of the ocular surface (such as the one provided by the Cassini topographer), in which the most curved meridian can be clearly seen and details of the limbus can be distinguished, and on the side of the more sophisticated techniques, we can use other systems. The ones I have experience with are Alcon's Verion, Zeiss' Callysto and Truevision's Trueguide System (see images).
[caption id="attachment_2908" align="aligncenter" width="700"] Fig. 3. One can clearly distinguish the more curved meridian and the limbus input markings and then align the IOL in appropriate manner using only this image. Fig. 4. Alcon's Verion system.[/caption].
Is toric IOL implantation advisable to treat astigmatism in patients suffering from keratoconus or after corneal transplantation? As long as in both situations, keratoconus and post-corneal transplantation, the astigmatism is stable (no change in a minimum period of 12 months) and the regular component is prevalent (if the irregular component is significant, the best corrected visual acuity with spectacles will be significantly lower than the best corrected visual acuity with a rigid gas permeable contact lens and should not be higher than a Snellen line in an ideal indication), I believe we have sufficient support in the currently published data to use pseudophakic toric IOLs in these patient subgroups.
Corneal astigmatism can, of course, change over the long term (as can also happen with age in normal, unoperated eyes), but the superiority in results concerning uncorrected vision, and thus quality of life, is so significant that I am among the surgeons who support their use in the circumstances described above.
Of course we have to explain well to our patients the possibility of future changes, as well as the different treatment options that we will consider if this occurs: from using an additional correction (with glasses or contact lenses) to evaluating a further surgical procedure, if not contraindicated (laser, refractive surgery, IOL replacement, anterior or posterior chamber 'piggy-back' IOL). Theoretically, in the near future, we will have the possibility of changing the power of the IOL in situ with new technologies that are currently being developed and tested.
What is the astigmatism cut-off value for recommending cataract surgery with a toric IOL? In fact, I use pseudophakic toric IOLs in most of my cataract patients when the net corneal astigmatism is equal to or greater than 1 D. Probably in the near future, when the general refractive predictability of cataract surgery improves, this cut-off value will be lower.
José L. Güell, MD IMO- Instituto Microcirugía Ocular
Associate Professor of Ophthalmology
Autonomous University of Barcelona (UAB) - Spain
E-mail: guell@imo.es
Please note that cookies are installed on this site by us and our selected partners to collect and process personal data from your devices (e.g. IP address, precise device tracking and geographical location),
Your consent is not required for the installation of technical and necessary cookies. For the others, however, you can freely give, refuse and revoke consent for the installation of all or some of the tracking systems and change your preferences by accessing the "Manage" section, which can be reached through the Cookie Policy or through this banner.I acceptI do not acceptRead more
You may revoke your consent at any time by using the Revoke Consent button.I want to delete cookies