







The development of micro-incision is undoubtedly one of the most important frontiers in the advancement of cataract surgery. In order to understand its advantages and prospects for further development, we interviewed one of the leading experts in the field: Dr. Roberto Bellucci, Director of Hospital Ophthalmology at the Azienda Ospedaliera Universitaria Integrata di Verona.
 What is Micro-incision in Cataract Surgery?
What is Micro-incision in Cataract Surgery?
MICS stands for Micro Incision Cataract Surgerya technique in which cataracts are removed through an incision of 2 mm or less.
The term was coined by Spanish colleague Jorge Alio, and has since spread throughout the world. Originally, there were two MICS techniques, considered alternatives: the biaxial technique separated irrigation from suction and used standard 1.1 mm phaco tips, while the coaxial technique used reduced phaco tips and sleeves. It was later realised that the two techniques are too different to be lumped together under the same label, so at present it is commonly understood to be MICS only the coaxial technique.
What equipment does it require?
Initially introduced to reduce the size of the incision, the MICS technique has undergone so many developments that it is now considered a stand-alone technique, and equipment has rapidly adapted to the new surgical conditions.
- The phaco tip is small, with an internal lumen of 0.5 mm in diameter. Such a tip must be trumpet-shaped ('flared') and have an angled cutting edge to face masses with as large a surface area as possible. In fact, pressure (and also depression or suction) is the force multiplied by the surface area and increases with it. A small drill bit, however, tends to clog, and then the suction force (the 'vacuum') must be greatly increased. Furthermore, the thinness of the metal makes it less durable, which is why there are even disposable tips. The thin body of the tip favours irrigation.
- The sleeve is also reduced and its fragility recommends single-use only. The sleeve also only irrigates on the sides due to the shape of the phaco tip, reducing the tendency to repel masses.
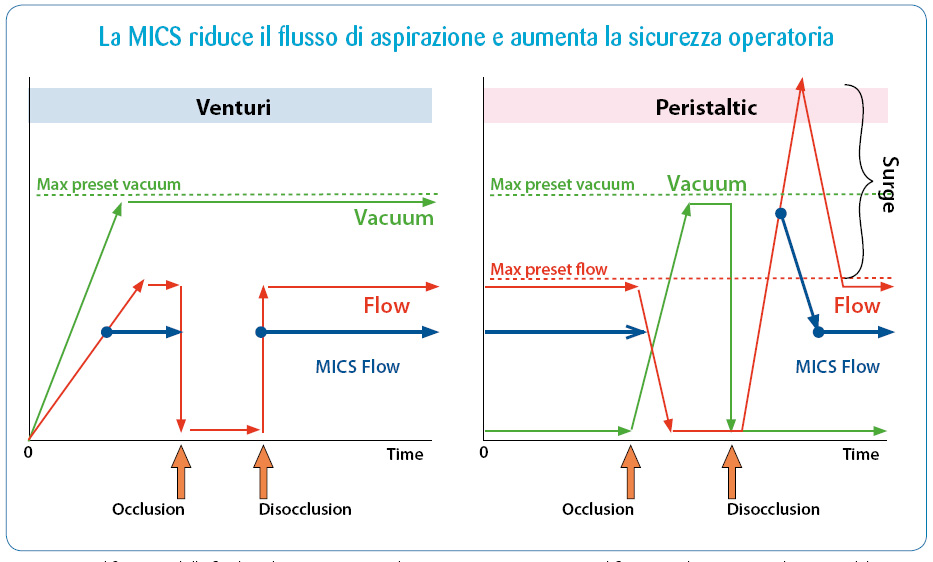
- The suction line must have absolute volume rigidity, achieved by means of small, short tubes that reduce the 'surge' effect, the extra suction that develops upon disocclusion and tends to collapse the chamber. In some systems, cataractous masses are retained by a filter located near the handpiece, preventing cataractous masses hydrating along the line from eventually clogging it.
- The phaco pump must have a very low hysteresis in order to respond immediately to the surgeon's commands and prevent the chamber from collapsing.
- Venting must be very efficient, and it really is in the new machines.
- Intraocular lenses must be designed for MICS. In particular, the new generation of hydrophilic acrylic lenses, which can be injected through incisions of 1.8 mm and smaller, are excellent. The 'compression' they receive in the cartridge causes them to squeeze out a little water, which is then immediately regained after implantation.
When these elements are optimised, the fluid balance is set at lower irrigation and suction levels than with traditional phaco, and the pressure in the anterior chamber during surgery does not rise to the levels we are used to. My bottle is never more than 60 cm high, and the chamber never collapses: the reduced suction lumen only allows a reduced flow, while the depressions remain high above the usual.
Why is it better than the normal phaco?
MICS is always better than normal phaco. The incisions are smaller and alter the cornea less; intraoperative fluidics is better and safer, with reduced anterior chamber pressures and fewer collapses; cataract removal is faster and more progressive; intraoperative complications are fewer; and the postoperative is smoother and more satisfactory. However, I believe that the stability of the anterior chamber with the reduced collapse complications is the most important advantage of MICS. For me MICS does not mean a small incision, but a better and safer way of operating cataracts.
Why is it not yet universally popular?
A number of reasons hinder the spread of MICS, ranging from the traditionalist tendency of many of us surgeons to increased costs, from lack of awareness of the benefits to the apparent goodness of traditional techniques.
I myself switched to MICS out of curiosity rather than conviction, the enthusiasm came as I realised the enormous advantages of MICS.
Let's just think about teaching: we had a resident who in his first year of specialty started operating with MICS, the best technique for teaching and learning.
What will be the next developments?
Phaco and lens technology have been playing tennis for 30 years, bouncing the ball. I think it is now the turn of lenses, and we see new products all designed for MICS all the time. For example, the new Mini lens range from Sifi MedTech is excellent in this respect, a real step forward for Italian industry and technology.
Conclusion: should we abandon classical techniques?
But we have already abandoned them!
Only MICS is available in the Verona hospital, we no longer have 1.1 mm tips, and we certainly don't regret them!
Surgical times did not lengthen (still 20-22 operations per day, while the other room does retina, cornea and glaucoma), complications were reduced, patient satisfaction increased.
Dr. Carmelo Chines
Direttore responsabile