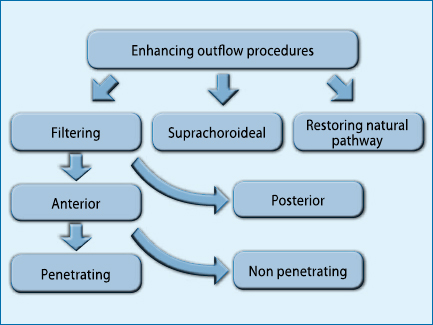
In recent years, glaucoma surgery has been the subject of renewed interest, with the emergence of new types of surgery and the reappraisal of the ab interno approach.
drainers, valved and non-valved), depending on whether the aqueous humour is drained at the anterior or posterior portion of the bulb. Anterior filtering can then be divided into penetrating (e.g. trabeculectomy) and non-penetrating (e.g. deep sclerectomy), depending on whether or not there is a direct entrance into the anterior chamber (Fig. 1).
All these procedures, with the exclusion of non-perforating anterior filtrations and posterior filtrations, can be performed with either an ab external or ab internal approach.
Cyclo-destructive procedures are generally reserved for the very advanced or terminal stages of refractory forms, with the main aim of reducing or avoiding algic symptoms. The question that arises is: why, if surgical treatment provides better control of endocular pressure, is it generally reserved for cases where medical therapy is insufficient to ensure adequate tonometric control?
The answer lies in the fact that anterior filtrations are subject to a non-negligible incidence of failure and complications. The inconstancy of results can be summed up in the fact that filter surgery, despite all the improvements made over the years, still remains an operation where 'a hole is drilled in the eye hoping that it will work, but not too much'. The statement is brutal but, although it does not account for the improvements made to the original technique described by Cairns, it has its own kernel of truth, which lies mainly in the variable of individual scar response.
Various important modifications to the original trabeculectomy technique have been made in order to reduce failures and increase safety.
[caption id="attachment_1556" align="aligncenter" width="436"]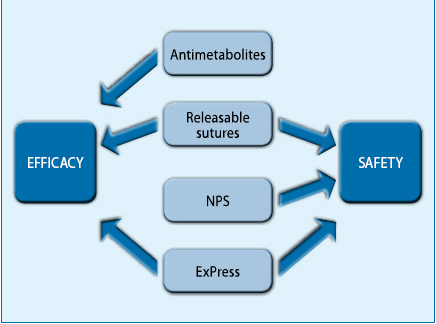 Fig. 2. Variants on the Cairns technique.[/caption]
Fig. 2. Variants on the Cairns technique.[/caption]
The most significant variants (Fig. 2) include:
1. L'use of antimetabolites, aimed at increasing the effectiveness of the intervention. These drugs are now indispensable in most cases, given the inflammatory changes induced in the subconjunctival tissue by prolonged topical therapies, which have led to a significant increase in the number of failures. Despite attempts at standardisation, the use of these (off-label) drugs suffers from a considerable amount of empiricism and can lead to serious complications even after some time.
2. Le releasable suturesat the level of the external scleral flap. Such sutures if properly placed and tightened strongly reduce filtration in the immediate postoperative period, allowing it to increase upon release. Reducing filtration in the immediate postoperative period is essential, as most complications occur in the immediate postoperative period and are generally related to hypotonia. In addition to eliminating hypotonia, good closure of the scleral flap reduces the production of second-forming aqueous, which is rich in factors stimulating healing, and increases the chances of success.
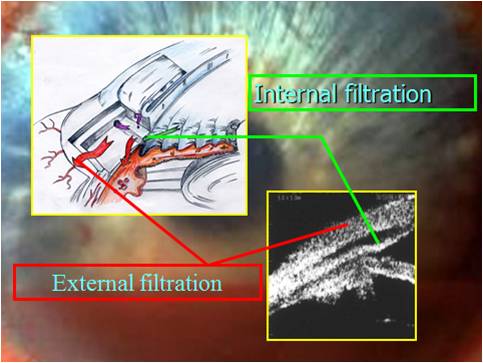
[caption id="attachment_1557" align="alignleft" width="300"]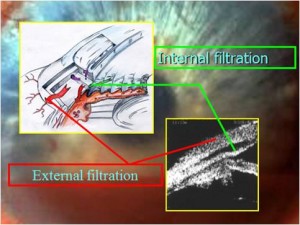 Fig. 3. The deep sclerectomy.[/caption].
Fig. 3. The deep sclerectomy.[/caption].
3. The non-perforating surgerywhich was also created to reduce postoperative complications related to hypotonia. In this surgery, the trabeculodesematous membrane is left in situ, which constitutes a further point of filtration regulation. Thus, in these patients we have an internal filtration (from the anterior chamber to the scleral lake through the trabeculodesematous membrane and an external filtration (from the scleral lake to the subconjunctival space similarly to all anterior filtrations). The technique undoubtedly increases safety, but requires close and accurate follow-up as the filtration points are now 2 (Fig. 3) and any one of them can become blocked giving a hypertone; in such a case, for an adequate therapy, it is necessary to identify the site of the blockage (external or internal) by gonioscopy and ultrabiomicroscopy and intervene accordingly.
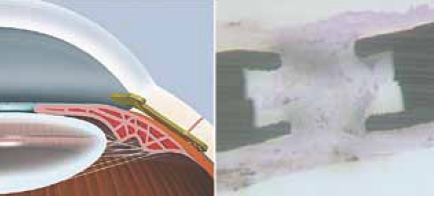
4. The armed surgerythe use of ExPress. The ExPress is basically a small drilled nail that is directly implanted under the scleral flap, replacing the surgical time of the trabeculectomy and eliminating the iridectomy. This has the advantage of working practically with a closed chamber (avoiding intraoperative complications such as, for example, the incarceration of the iris at the trabeculectomy site), of guaranteeing a constant flow (eliminating the variability due to the size of the trabeculectomy) and of reducing the incidence of haemorrhages and phlogosis in the anterior chamber, having avoided creating a real surgical wound in direct communication with the anterior chamber (Fig. 4).
Personal experience led me to choose the ExPress implant in combination with the use of antimetabolites and releasable sutures as the best compromise in terms of safety, effectiveness and simplified follow-up.
[caption id="attachment_1558" align="aligncenter" width="438"]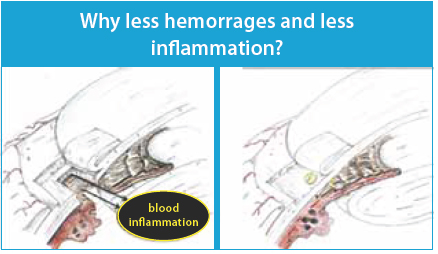 Fig. 4. Left: trabeculectomy. Right: Express implant[/caption].
Fig. 4. Left: trabeculectomy. Right: Express implant[/caption].
The possibility of performing ab interno anterior filtration surgery after Worst's attempts is now the subject of new attention with a collagen tubular insert (Fig. 5 Aquesys), which looks very promising, at least from a theoretical point of view, but which, being in the experimental phase, has no significant data.
[caption id="attachment_1559" align="aligncenter" width="433"]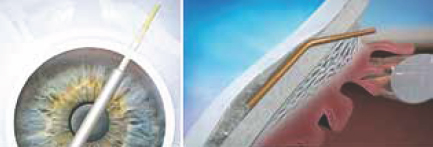 Fig. 5. Aquesys. Left: ab-interior plant. Right: operation diagram.[/caption]
Fig. 5. Aquesys. Left: ab-interior plant. Right: operation diagram.[/caption]
Le rear filtersThe use of valved and non-valved drainage inserts, until recently considered the last resort, is now being re-evaluated against trabeculectomy in relation to recent evidence in the literature.
In this type of surgery, the aqueous humour is diverted into the posterior subtenonian space; with this premise, fibrin glue can be used in the anterior portion of the bulb, resulting in a perfectly watertight tissue closure and minimising the chances of hypotonia in the early postoperative period.
The limitations of posterior filtering basically lie in the antiquity of the currently available implants, which, having been designed around 20 years ago, have characteristics that are not in keeping with modern microsurgery: for example, we need only recall how the entrance to the anterior chamber is made with a coarse silicone tube.
The suprachoroidal pathway
Postulated by Heine in the early 1900s, taken up by Strampelli in the 1960s with the cyclodiastasis, effective intervention but burdened with an unacceptable complication rate, has known new life with the Gold Shunt and the CyPass. The Gold Shunt, in its various versions, is basically a gold draining insert that is inserted ab externally with one end in the anterior chamber and one end in the suprachoroidal space.
Personal experience in this regard (more than 80 cases) has shown that after discrete results in the short to medium term, failure occurs
[caption id="attachment_1560" align="alignleft" width="300"]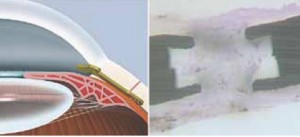 Fig. 6. On the left the Gold Shunt. Right Histological preparation of excised Gold Shunt: fibrosis surrounds and invades the shunt in its distal portion.[/caption]
Fig. 6. On the left the Gold Shunt. Right Histological preparation of excised Gold Shunt: fibrosis surrounds and invades the shunt in its distal portion.[/caption]
mainly by scarring in the suprachoroidal space (Fig. 6). This space has been mistakenly considered by some to be a poorly reactive space: it is instead a space outside the blood-ophthalmic barrier, richly vascularised and characterised by a strong fibroblastic response to the surgical insult.
The CyPass inserted with an ab interno procedure (Fig. 7), which is much less traumatising than the ab esterno procedure of the Gold Shunt, has shown discrete results in the short term, but there is a lack of controlled studies verifying its efficacy over time, and although the postoperative inflammation induced is significantly less than with the Gold Shunt,
may have the same fate in the long term.
[caption id="attachment_1561" align="aligncenter" width="432"]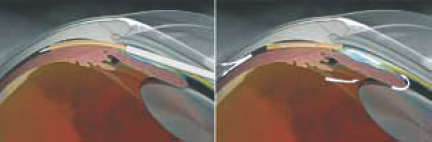 Fig. 7. CyPass insertion.[/caption].
Fig. 7. CyPass insertion.[/caption].
l restoration of natural drainage routes
The removal of the obstacle present at the trabecular level can be performed with ab externally and ab interno procedures. Of the ab external procedures, the most commonly performed is undoubtedly the canaloplastyan evolution of viscocanalostomy. Canaloplasty is a complex operation which, like all ab externo operations, engages a considerable portion of the conjunctiva of the upper quadrants (an element to be taken into account in the event of the need for re-intervention due to failure) and whose results in the literature are comparable to those of non-perforating filtrations. A simplification currently being studied is the use of the Stegman's canalicular dilators which are implanted in Schlemm's canal instead of prolene wire.
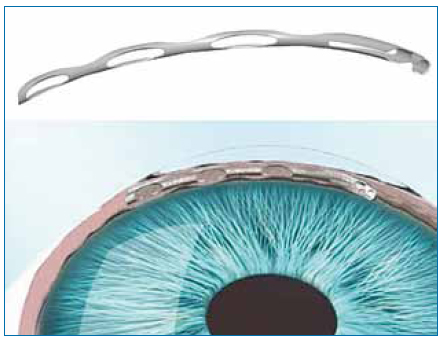
[caption id="attachment_1562" align="alignleft" width="300"]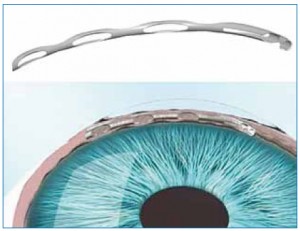 Fig. 8. The CyPass.[/caption]
Fig. 8. The CyPass.[/caption]
The ab interno procedures, on the other hand, are numerous: the best known are the Trabectomeand canalicular installations iStent and Hydrus. Of these Trabectome and iStent have been approved by the US FDA while the more recently introduced Hydrus seems to give the best results in my experience. It is a nitinol stent (Fig. 8) that is inserted into Schlemm's canal by gonioscopy and keeps it dilated; its length (8 mm) gives it the advantage over the iStent (1 mm) of acting on a longer portion of the canal with a greater chance, if not certainty, of affecting parts where collector canal orifices are present.
Conclusions
Ab interno procedures have significant advantages over ab esterno procedures:
- the reduced traumaticity: the postoperative course is generally very quiet, comparable to that of a phacoemulsification.
- The very rapid functional recovery.
- The reduced incidence and severity of complications: in this regard, it should be emphasised that even in the case of incorrect positioning of the stent in the ciliary body, no devastating complications have been reported, only the non-functioning of the stent itself. The most frequent complication is a slight blood effusion in the anterior chamber, which at most persists for a few days.
- Conjunctiva sparing: which always leaves the option of traditional filtering surgery in case of failure.
- The absence of a filtering draft, for procedures involving Schlemm's canal or the suprachoroidal space.
- The speed of the intervention itself, which takes only a few minutes.
[caption id="attachment_1563" align="alignleft" width="300"]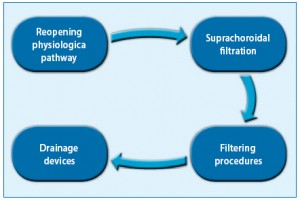 Fig. 9. Hypothetical treatment algorithm.[/caption].
Fig. 9. Hypothetical treatment algorithm.[/caption].
Significant may be the fact that most patients operated with these techniques request the same operation for the second eye. Conversely, it must be reported that gonioscopic techniques are unusual for most surgeons, who may be initially uncomfortable. However, it is clear that the ab interno approach has great advantages and enormous possibilities for development, and its spread will be facilitated by the development of new instruments for visualising the camerular angle.
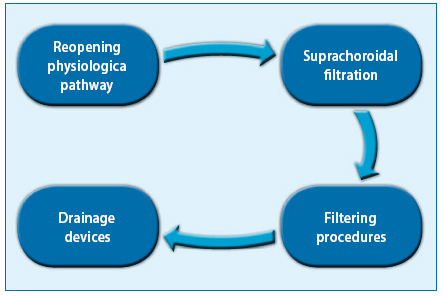
With this in mind, one can try to hypothesise what could probably be the treatment algorithm in the near future (Fig. 9). Where possible, the first approach will be with ab interno techniques to restore the natural outflow pathways, followed in case of failure by an ab interno approach in the suprachoroidal space, followed in turn by an anterior filtration (ab external or ab interno) and finally by a posterior filtration in case of failure of the previous ones.
The future looks, therefore, fascinating and we could conclude like Sir Winston Churchill: 'Now this is not the end. It is not even the beginning of the end. But it is, perhaps, the end of the beginning'.
Marco Nardi
Dr. Carmelo Chines
Direttore responsabile








 The only treatment with proven efficacy for glaucomatous disease is the reduction of intraocular pressure in order to halt or slow down the progression of functional damage; it is also known that surgical treatment, when successful, allows more effective control of eye pressure than pharmacological treatment.
The only treatment with proven efficacy for glaucomatous disease is the reduction of intraocular pressure in order to halt or slow down the progression of functional damage; it is also known that surgical treatment, when successful, allows more effective control of eye pressure than pharmacological treatment.