







Keratitis by Acanthamoeba (CA) is a rare but potentially devastating infection. The main risk factor for infection with Acanthamoeba is the prolonged and incorrect use of contact lenses - for example, it is not correct to wear them while bathing or showering and their cleaning should not be carried out with running water. Further risk factors are damage to the corneal surface and exposure to contaminated water.
But what is theAcanthamoeba? and how does it cause infection in the eye?
L'Acanthamoeba is a ubiquitous protozoan, i.e. present in various environments, including air, soil and water. The life cycle of this microorganism consists of two biological forms, a cyst - normally dormant and highly resistant to antibiotics and adverse conditions - and a trophozoite - the cell in its state capable of infecting the host.
In case of corneal infection, Acanthamoeba binds to the corneal epithelial cells through various proteins; this binding results in toxic effects on the corneal epithelial cells themselves and supports the penetration of the microorganism into the deeper layers. At this point, Acanthamoeba is also able to migrate along the corneal nerves and damage them, so much so that some patients ultimately have to resort to corneal transplantation.
Signs and symptoms from Acanthamoeba keratitis
In the case of CA, the most common symptoms are similar to those of other eye infections: severe pain, redness and irritation in the eye, visual disturbances, hypersensitivity to light and excessive tearing. These symptoms may persist for several weeks.
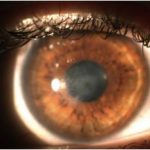
I clinical signs of CA are varied and range from epithelial changes (e.g. epithelial microerosions and microcysts) to the presence of different types of infiltrates (e.g. multifocal stromal infiltrates and peripheral perineurial infiltrate).
Corneal infection with Acanthamoeba can also lead to the onset of complications, some common (broad-based anterior synechiae, secondary glaucoma, iris atrophy, persistent mature endothelial defect cataract), while others are rarer (anterior sterile uveitis, scleritis, chorioretinitis and retinal vasculitis).
Precisely because many of the signs and symptoms that sufferers present with this infection may appear similar to those due to other types of keratitis, CA may be misdiagnosed and treated like other types of keratitis (herpetic, bacterial or fungal). This delay in diagnosis, as well as the use of inappropriate treatment, has a negative impact on the patient's clinical course.
A recent study evaluated how several factors (the stage of the disease of patients with CA, the time from the onset of keratitis to appropriate treatment, the time to clinical resolution and visual acuity) can critically influence the healing time. The results showed that the overall healing time of patients with CA was approximately 9 to 15 months, whereas patients who also had a severe corneal ulcer (stage III CA) had a significantly longer healing time.
 In particular, patients who received early treatment (within 30 days of symptom onset) had a shorter recovery time than patients with delayed diagnosis. The study also assessed quality of life approximately 11 years after the onset of symptoms. The study found that the disease, even many years later, reduced this important parameter due not only to the sequelae of AC, but also due to the long recovery time, characterised by severe daily pain with recurrent acute episodes, as well as the need for frequent treatment and lengthy follow-up. However, it is important to emphasise that patients who were diagnosed early showed a lower reduction in quality of life than patients diagnosed late.
In particular, patients who received early treatment (within 30 days of symptom onset) had a shorter recovery time than patients with delayed diagnosis. The study also assessed quality of life approximately 11 years after the onset of symptoms. The study found that the disease, even many years later, reduced this important parameter due not only to the sequelae of AC, but also due to the long recovery time, characterised by severe daily pain with recurrent acute episodes, as well as the need for frequent treatment and lengthy follow-up. However, it is important to emphasise that patients who were diagnosed early showed a lower reduction in quality of life than patients diagnosed late.
Patient journey: how the diagnosis of A-keratitis is madecanthamoeba?
In case of clinical signs of AC, the ophthalmologist will perform some or all of the following examinations:
- molecular analysis of corneal scrapingsIt has a very high sensitivity and can give a result within 60 minutes. However, this test can have the disadvantage that even the presence of genetic material from the non-living micro-organism can give a positive result
- confocal microscopy in vivo: has a higher sensitivity than 90% when performed by experts; however, with this method only cysts of Acanthamoeba are well recognisable
- cultivation in vitro: has variable sensitivity and has the disadvantage of giving results after 3 weeks
- histopathological analysis: has a discrete sensitivity and corneal scrapings or excision or excised tissue from keratoplasty can be analysed.
Treatment of Acanthamoeba keratitis: what's new?
Effective treatment requires the eradication of the resistant encysted form, as well as the more susceptible form, trophozoite. There is currently no drug approved specifically for CA. The most widely used treatment is based on the instillation of biguanide eye drops, either as monotherapy or with the addition of a diamidine.
Several data, however, indicate that polyhexanide monotherapy for the initial treatment of CA is as effective as biguanide + diamidine combination therapy.
Regarding the use of polyhexanide, a recent study evaluated the safety of polyhexanide-based eye drops at different concentrations (0.04%, 0.06%, 0.08%) and showed no significant differences in tolerability between treatment groups. The results of this study laid the foundation for further exploration of the efficacy of polyhexanide 0.08% treatment in a larger phase III study (ClinicalTrials.gov Identifier: NCT03274895), the results of which will be available as soon as the study is completed.
The eventual availability of a drug specifically indicated for CA would be a big step forward for the health of patients suffering from this disease.
Bibliography
- Bonini S, Di Zazzo A, Varacalli G, Coassin M. Acanthamoeba Keratitis: Perspectives for Patients. Curr Eye Res. 2020 Nov 29:1-6.
- Szentmáry N, Daas L, Shi L, Laurik KL, Lepper S, Milioti G, Seitz B. Acanthamoeba keratitis - Clinical signs, differential diagnosis and treatment. J Curr Ophthalmol. 2018 Oct 19;31(1):16-23.
- Pope V, Rama P, Radford C, Minassian DC, Dart JKG. Acanthamoebakeratitis therapy: time to cure and visual outcome analysis for different antiamoebic therapies in 227 cases. Br J Ophthalmol. 2020 Apr;104(4):575-581.