







L'Oculista Italiano adheres to World Diabetes Day by sharing with its Readers not only articles dealing with eye diseases, but also important updates on scientific advances concerning diabetes, a chronic disease that can lead to serious eye complications.
Precision medicine, better known by the term ''precision medicine''.personalised medicine", is gaining momentum in an era of health revolution that is being called "tailored-patient"i.e. patient-centred. Precision medicine is, in fact, a new medical approach that takes into account the genetic, environmental and lifestyle variability of each individual in order to improve the prevention but especially the treatment of diseases. This new way of approaching the disease actually began to take hold in 2015 in America, when the then US President B. Obama, launched a campaign to support research based precisely on precision medicine for the treatment of oncological and diabetic diseases. Precision medicine, in fact, makes it possible to improve and optimise drug therapy that is often ineffective on certain subjects, and is also able to limit certain side effects. Clinical evidence on diabetic pathology, for example, has shown that not all individuals with type 2 diabetes (DMT2) respond to therapy in the same way. Hence the need to correctly redefine the types of diabetes in order to achieve a more accurate diagnosis and increasingly customised therapy.
Sub-classification of type 2 diabetes
Traditionally, the classification of diabetes has been based solely on the concentration of a single metabolite, glucose. Based on this parameter, diabetes was classified into two forms: type 1 diabetes mellitus (DMT1, insulin-independent) and type 2 diabetes mellitus (DMT2, insulin-dependent). However, to date, this subdivision is not very exhaustive, especially considering the different forms that DMT2 can take. In particular, DMT2 is subdivided into:
–LADA (Latent Autoimmune Diabetes in Adults), a form of autoimmune diabetes that arises in adults;
–MODY (Maturity Onset Diabetes of the Young), a form of hereditary non-autoimmune diabetes that manifests early;
–neonatal diabetesa diabetic form that arises in the neonatal period.
Monogenetic forms, i.e. due to the mutation of single genes (MODY and neonatal) have paved the way for a new approach based not only on blood glucose levels (insulin or non-insulin dependent diabetes), but on other parameters.
A recently published European study by a team of researchers from the University of Finland and Sweden classified five subgroups of patients (over 18,500,000 subjects) with DMT2 based on six different variables, including age at diagnosis and body mass index. I 5 subgroups were:
Severe autoimmune diabetes (SAID, severe autoimmune diabetes), patients with high levels of GADA (glutamic acid anti-decarboxylase) autoantibodies, low insulin levels and low glycaemic control;
2.Severe insulin-deficient diabetes (SIDD, severe insulin-deficient diabetes), patients with low levels of insulin secretion, low glycaemic control and high risk of developing diabetic retinopathy;
3.Severe insulin-resistant diabetes (SIRD, severe insulin-resistant diabetes), patients with high levels of insulin resistance, obesity, late onset of diabetic disease and other risk of developing nephropathy;
4.Moderate obesity-related diabetes (MOD, mild obesity-related diabetes), obese patients, early onset and optimal glycaemic control;
5.Age-related moderate diabetes (MARD, mild age-related diabetes), patients with excellent glycaemic control and late diabetic onset.
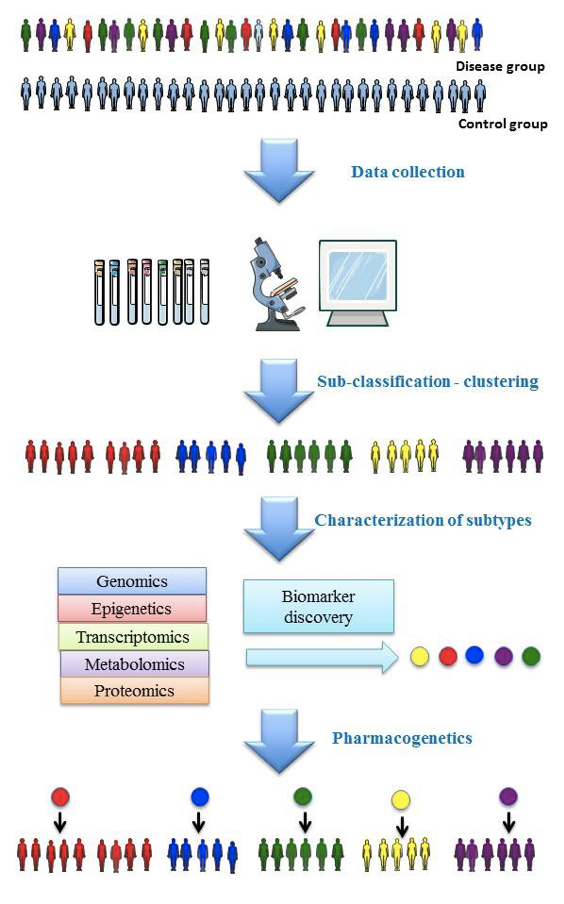
Image taken from Prasad RB et al. J Intern Med, 2018. doi:10.1111/joim.12859
This proposed classification of DMT2 sufferers into subcategories could, according to the authors, contribute to the implementation of precision medicine and identify the best treatment strategy for each patient.
In fact, in Depending on the categorisation into one of the five different subgroups, the therapy as well as the frequency of, for example, specialist visits to which DMT2 patients must undergo may vary: those belonging, for example, to group 4 or 5, do not need constant specialist visits, but can be more easily managed by adopting small lifestyle changes. It is therefore clear that this would also make it possible to significantly reduce the social and economic cost of this chronic disease.
Source
Prasad RB et al. Precision medicine in Type 2 Diabetes. J Intern Med, 2018. doi:10.1111/joim.12859.
Dr. Carmelo Chines
Direttore responsabile