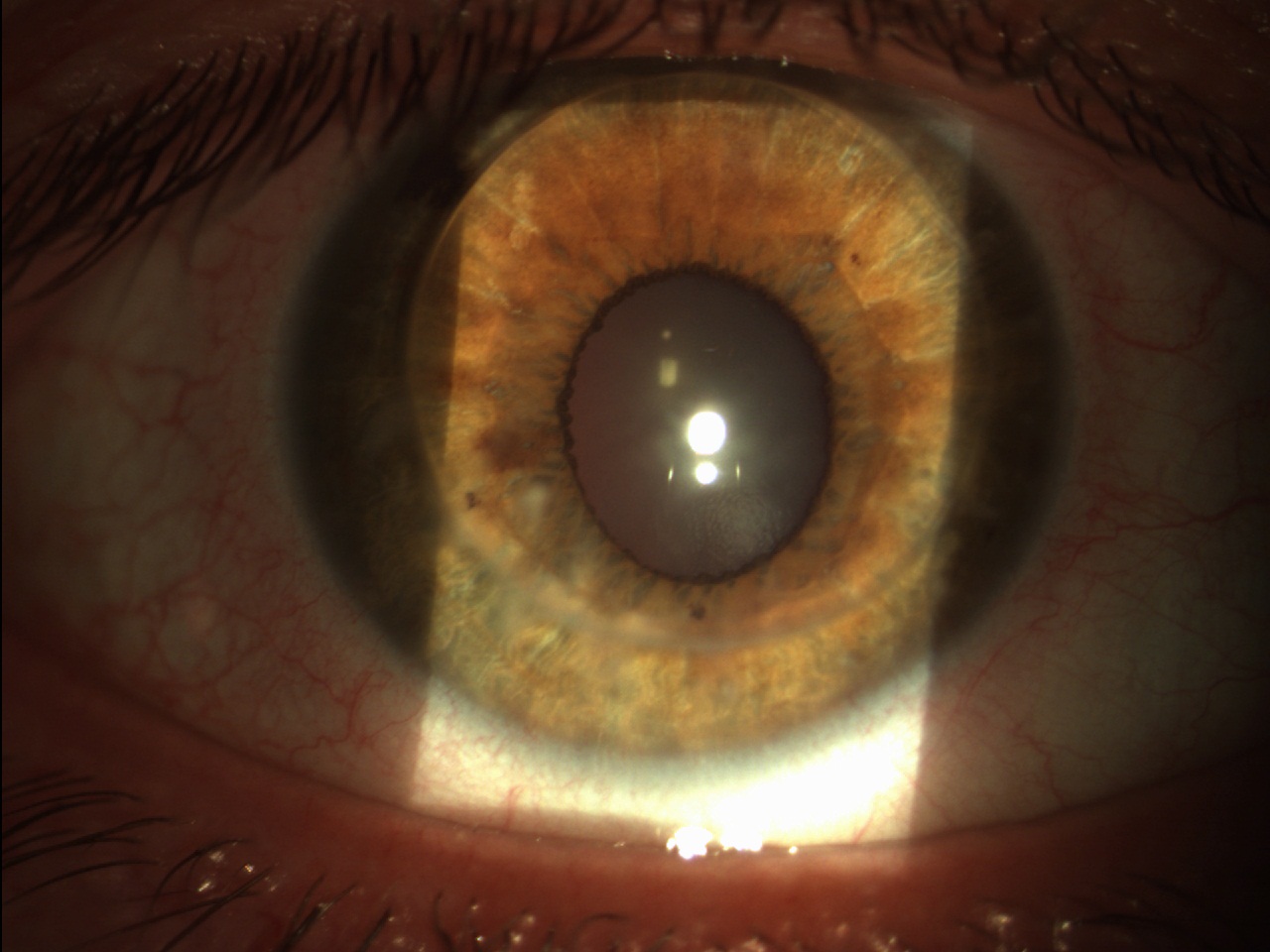
Toric intraocular lenses have become a standard in refractive cataract surgery. It has been proven that they can effectively compensate corneal astigmatism with very high precision. Specific surgical guiding systems and instruments for axis marking have evolved a great deal in recent years. A great advantage of toric IOL implantation is that one can, in fact, achieve the correction of almost any kind of astigmatism, even the correction of very high astigmatism, e.g. after PRK (Fig. 1).
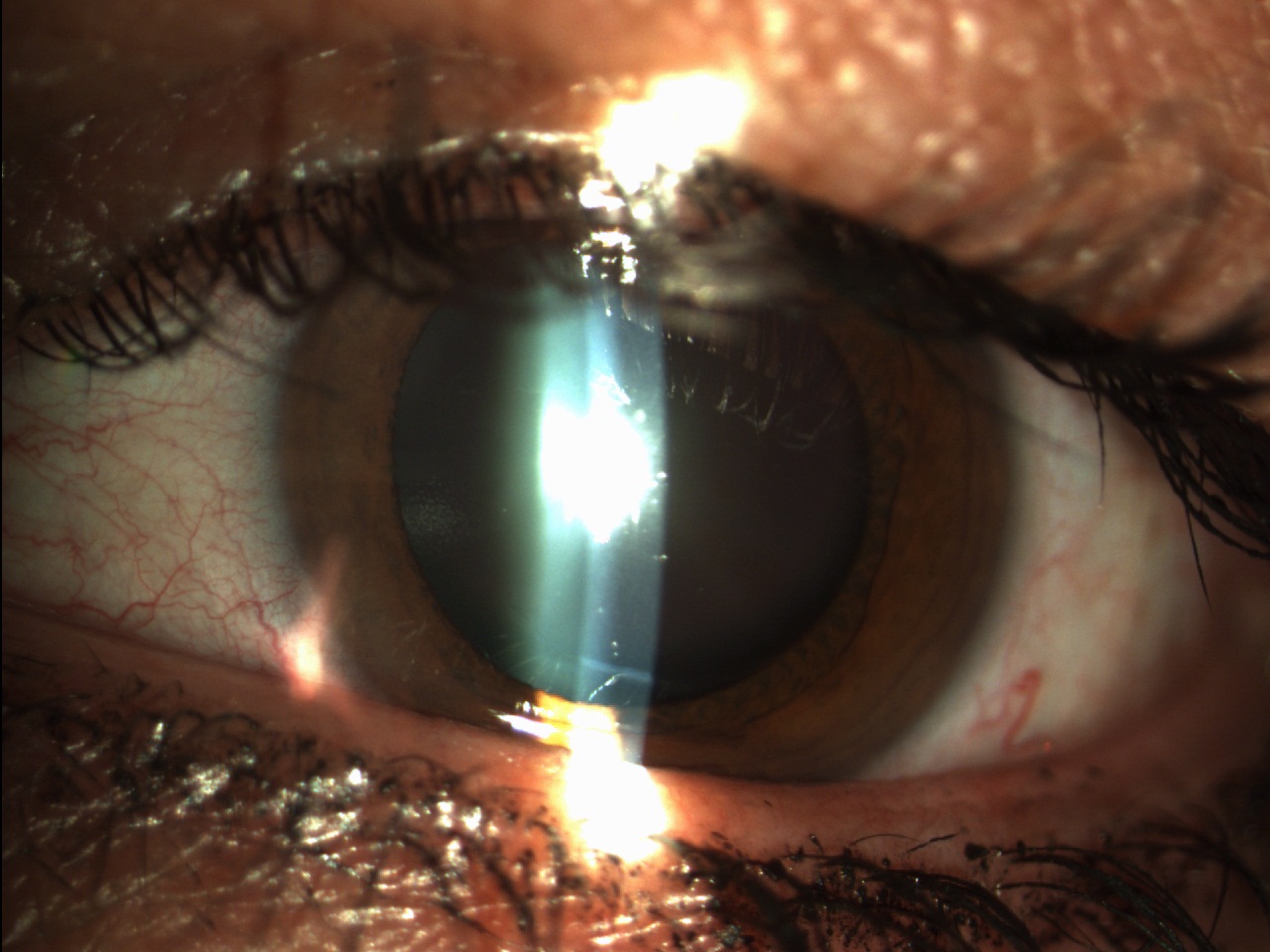
Especially in Europe, many companies offer customised toric IOLs. Toric IOLs are indicated from 1.0 to 1.5 diopters of astigmatism upwards. Below this value there is still room for manual or femtolaser astigmatic keratotomy (KA). The disadvantages of KA are a limited correction range and unsafe long-term stability. However, especially below 1.0 diopter, the incisional technique and KA are good alternatives. (Fig. 2).
What is the ideal match between pre-operative parameters and characteristics of Premium IOLs for cataract surgery with toric IOLs?
When the patient presents for pre-operative examination, it is not always clear whether he or she is a candidate for toric IOL or multifocal lens implantation Premium. In general, it is recommended to carry out keratometry with IOL Master/Lenstar or topography as the first measurement. If this measurement is taken at a later stage of the pre-operative examination, corneal changes will have already been determined due to the IOL measurement, the administration of eye drops and other corneal manipulations.
Patients should not wear contact lenses in the two weeks prior to corneal measurements. This can significantly influence the calculation of the toric IOL. The correction of astigmatism in the multifocal lens patient has been shown to produce excellent results in this class of subjects. These patients, in fact, greatly appreciate spectacle independence compared to patients who only have spherical ametropia
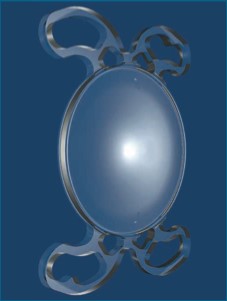
[caption id="attachment_3001" align="alignright" width="227"] Fig 3. Example of toric IOL with loop (B + L).[/caption]
Fig 3. Example of toric IOL with loop (B + L).[/caption]
Let us now address the problem of IOL rotation. How best to handle it: can 4 loops and a self-centring design be real advantages?
Rotation and misalignment of the toric IOL are fortunately not as common as many people think. The design of several IOLs has features that ensure full rotational stability. Included in this is a specific loop design (four loops, specific loop shape), as well as material adhesiveness. (Fig. 3) However, the design of the loops is extremely important for long-term outcomes as changes in the capsular bag can lead to decentralisation of the IOL or tilt and therefore the design of the loops should adapt to these changes.
Hi-tech design & premium IOLs: how important is technology for the best performing toric IOLs?
[caption id="attachment_3002" align="alignleft" width="226"]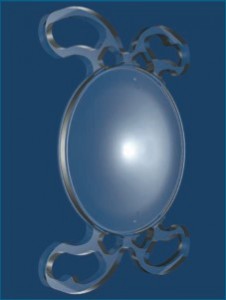 Fig. 4. 4-point IOL Mini TORIC (SIFI Medtech SRL - Italy)[/caption].
Fig. 4. 4-point IOL Mini TORIC (SIFI Medtech SRL - Italy)[/caption].
The best hi-tech design of a premium IOL is of no value when cataract surgery or lens removal itself leads to complications. A perfectly centred capsulotomy, a well-preserved capsular bag and a stable zonule are extremely important for the implantation of a toric IOL. Any signs of capsular bag damage or change can lead to decentralisation or rotation of the IOL. Furthermore, the positioning of the IOL along the correct axis should be ensured.
Cataract surgery with femtolaser can greatly influence the performance of toric IOLs. Surgical guidance systems, such as the Verion system and others available on the market, enable good axial alignment. Other approaches include axis marking with femtosecond lasers during femtophakic stages, particularly if the technology is linked to corneal topography and other measuring instruments.
However, an experienced surgeon can also use manual marking systems and standard phaco technology, which can also lead to excellent results with toric IOLs and premium toric IOLs (Fig. 4).
Gerd Uwe Auffarth
Dept. of Ophthalmology
Ruprecht-Karls University of Heidelberg - Germany
E-mail: auffarthg@aol.com
Read this interview in English
Dr. Carmelo Chines
Direttore responsabile