Ruptured ocular capillaries are a fairly frequent occurrence that often resolve without treatment, but can be an indicator of more important pathologies.
Experience and knowledge in cataract surgery with toric IOLs
Pubblicato il
Argomento
Surgical Area
An appropriate assessment of the complex problems associated with dhe cataract with toric IOLs presupposes a high caseload, with both simple and complex cases, filtered by a critical judgement resulting from in-depth knowledge. For this reason, we asked the Professor Ozana Morarualso well known in Italy as a speaker at countless ophthalmology congresses in our country.
Who is the patient candidate for refractive cataract surgery in the second millennium: expectations, cultural level, lifestyle? Nowadays, patients are more determined to achieve spectacle independence after cataract surgery and even explicitly demand it, even if they do not have cataracts - which means that they require refractive surgery treatment to resolve their ametropia. Precisely because of these high expectations, the IOL industry and refractive surgery, speaking generally, have undergone enormous development over the last 15 years or so.
Today, there are possibilities for correcting astigmatism through the implantation of a toric IOL, or for correcting presbyopia through a multifocal or trifocal IOL, and for the simultaneous correction of presbyopia and astigmatism, toric multifocal IOLs or toric trifocal IOLs are used.fine tuning) by resorting to laser technology to correct an unwanted refractive residue post-operatively. For larger 'refractive surprises', or for patients for whom laser corneal surgery is not a good option, there is IOL technology "Add-on" developed in recent years, which is useful for achieving the desired post-operative refraction, the so-called 'Plano refraction'.
By mastering all these new instruments and devices, therefore, the surgeon is able to offer his patients complete independence from spectacles, so much in demand nowadays, when patients are increasingly demanding, in line with the modern lifestyle.
Mini-incision and preloaded injector: what is their relevance to surgical outcomes? The smaller the incision, the less astigmatism is induced, but is there a downward limit? Clinical practice and studies have shown that an incision smaller than 1.8 mm has no real influence on astigmatism. Therefore, it is not really relevant from the point of view of induced astigmatism to make an incision smaller than 1.8 mm. On the contrary, the larger the incision, the greater - and, at the same time, more variable - is the influence on induced astigmatism. As a logical consequence, a small incision, between 2.2 and 1.8 mm, ensures a smaller, less variable and more controlled astigmatism - an indispensable requirement in toric IOL implantation for an optimal post-operative refractive result.
At the same time, even without toric IOL implantation, MICS cataract surgery ensures a safer surgical profile: by operating in a closed system, greater stability is ensured during surgery (in terms of anterior chamber depth, IOP, posterior capsule stability) and, at the same time, there is a lower risk of intraocular infection.
Again, however: the incision should not be too small, such that it must be forced and enlarged during surgery or during IOL implantation, jeopardising the integrity of the IOL and/or the safe closure of the incision through the self-healing (spontaneous healing), resulting in the need for suturing at the end of the procedure! One or more sutures on the incision will result in high astigmatism and completely alter the initial emmetropic target calculations, because the SIA becomes very high and unpredictable in these cases!
Pre-loaded IOLs are much safer in this respect: they do not involve any manipulation and contamination of the IOL. In my clinical experience, I have noticed that a short learning curve is necessary for their implantation, with some not particularly relevant issues related to the release of the IOL in AC, but also to a certain enlargement of the incision caused by the implantation itself.
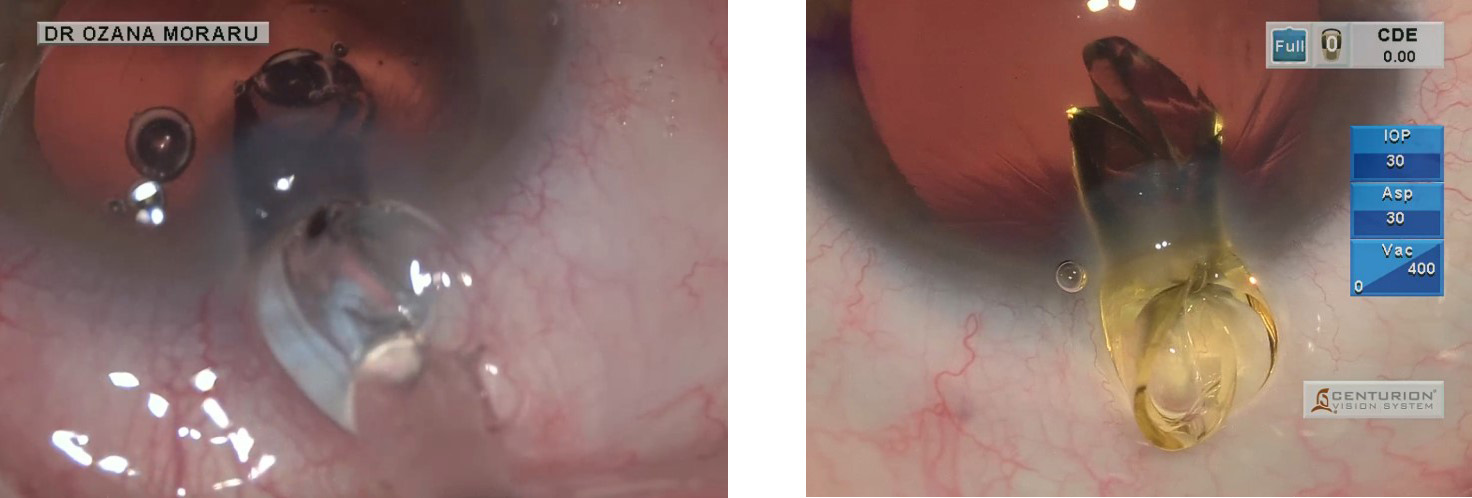
Figs. 1-2. Two different toric IOLs clamped in a 1.8 mm incision, resulting in a traumatic enlargement of the incision, with an increased and uncontrollable SIA and a possible lack of self-healing (spontaneous healing) at the end of the procedure, leading to the need for suturing.
On this topic, we will present at the ESCRS Congress in Copenhagen a study comparing implants of the Acrysof IQ IOL (Alcon) with three different devices (Cartridge type 'D' in a Monarch injector, Autosert System and Preloaded Ultrasert System), in which we compare three parameters: ease of implantation by technique 'wound assisted' (with possible complications during implantation), duration of the implant and enlargement of the incision by the implant itself. It seems that, at least in my direct experience, the System (UltraSert) preloaded with Acrysof IOLs widens the incision a bit more. This observation, and the associated result, can be important when we are targeting emmetropia, especially with preloaded toric IOLs, so we will need to change the value of the SIA Vector (Surgical Induced Astigmatism) in our toric calculation.
However, despite the initial learning curve and a certain widening of the incision, I believe that preloaded IOLs are safer in terms of surgical results, at least for safety reasons, due to the absence of manipulation of the IOL.
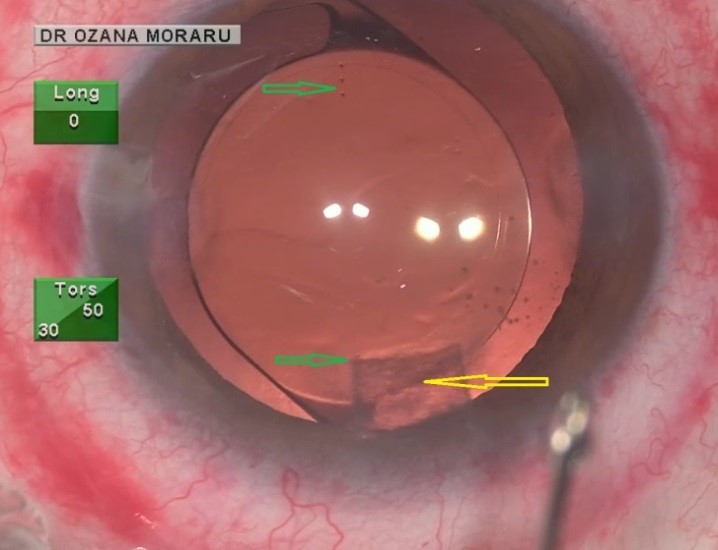
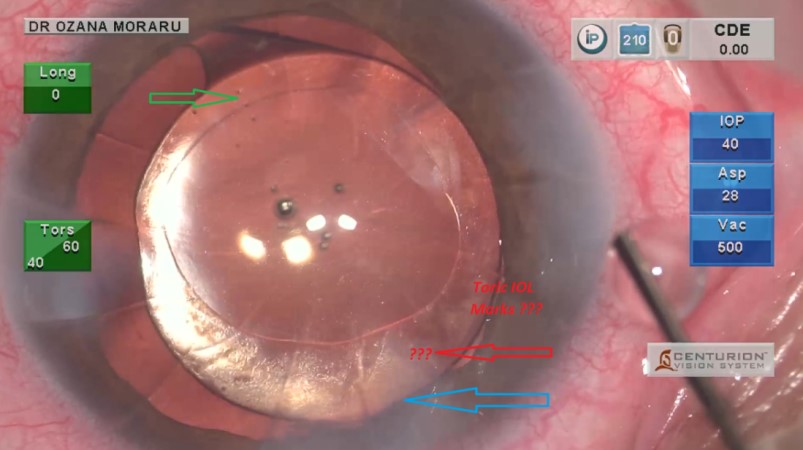
Fig. 3. A femtocataract procedure in which, despite the perfect incision made with the FemtoLaser (yellow arrow), the lack of transparency slightly compromises the toric IOL marking points in that area (green arrows).Leggi tutto
Why is the incision position so important for calculating the power of toric IOLs? As a general rule, theoretically, one might think that it is not so important since thoric calculator programmes can calculate the thoric position, without it mattering where the surgeon prefers to place the main incision. In practice, there are certain aspects that make the placement of the incision important and this issue is the subject of debate, with three main positions on this question:
– the first position suggests that the incision be made where the surgeon is most comfortable, and enter this into the Thoracic Calculator during the planning stage, so that the resulting calculation takes into account the location of the incision and gives a consequent T result.
– the second position is to always make the incision temporally, because the incision on the same axis always results in an SIA of the same value (more or less) - so it is more accurate and very easy to know - and because the SIA is minimised on the temporal axis: as it is already known, SIA and flattening effect of the incision are lower in a temporal approach than in a superior approach (by about a 50%), because of the different radial lengths of the cornea, on the horizontal axis and on the vertical axis; moreover, an superior incision is closer to the visual axis, in comparison with a temporal one, thus amplifying its flattening effect.
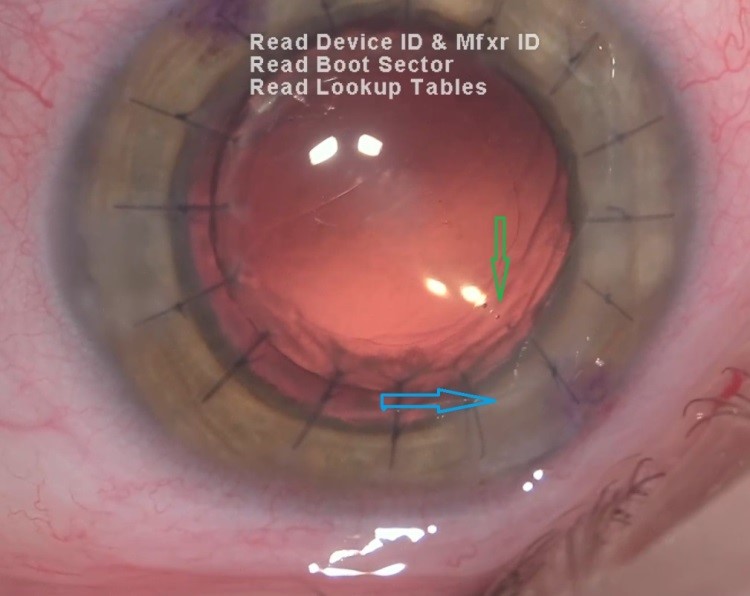
[caption id="attachment_2981" align="alignleft" width="300"] Fig. 4. Eye with previous radial keratotomies: the marking points (red arrow) are difficult to identify, compared to the lower ones, due to the main incision, located in the same place (blue arrow); radial keratotomies and epithelial cells of the anterior capsule increase the difficulty of visualising the marking points of the IOL.[/caption]
– the third position is to always make the incision on the most curved axis, as this approach will always reduce astigmatism; the disadvantage is that in this case, the surgeon needs to know his SIA on all meridians, which is not usually the case.
On the other hand, from a technical point of view, it seems to be a good idea to avoid planning the main incision on the same alignment meridian as the toric IOL, because corneal changes during or at the end of surgery (such as localised oedema) at the incision site may compromise good visualisation of the toric IOL marking points in that area.
Therefore, when the toric calculator provides us with a toric alignment below the incision site (Figs. 3-4), we should change the incision location in the toric calculator (but before surgery, in the planning stage, not in the operating room!), by 5-10 degrees from the proposed alignment of the toric IOL; this, clearly, will affect the induced astigmatism due to corneal changes. However, the toric calculator will modify the toric alignment axis accordingly and also its own value (Fig. 5).
[caption id="attachment_2982" align="alignright" width="300"] Fig. 5. Eye with previous penetrating keratoplasty in which the main incision (blue arrow) was planned correctly and made slightly off-centre from the marking point of the toric IOL (green arrow) - therefore the marking point is easily visible[/caption].
My personal preference is to always make the incision on the most curved axis when operating with non-torsic IOLs and always on the same axis when operating with toric IOLs: superiorly, at 100 degrees, where I am most comfortable. In this case, I choose the toric IOL with a greater correction of astigmatism (hyper-correction), to compensate for the greater astigmatism induced in the superior approach. As a rule of thumb, taking into account not only the higher astigmatism induced in the superior approach, but also the counter-rule effect of ageing, I under-correct the result by one T step in rule astigmatisms and over-correct by one T step in counter-rule astigmatisms.
There is only one exception, in terms of incision placement: in very high astigmatism, which requires a high toric power of the IOL, a value that exceeds the availability of toric powers on the market, or in cases of lack of 'just availability', I resort to some 'tricks', in order to increase the toricity effect of the IOL: by making a wider incision (a full-thickness opposing incision at plus/minus 180° distance), of about 2.8-3.5 mm practised on the most curved axis, so I can flatten that axis more, while increasing the effect of the toric IOL in the treatment of astigmatism.
I also practice the shorter incision tunnel in the cornea, so the flattening effect is even greater - it depends on the residual astigmatism values after the toric IOL effect, which needs to be corrected further.
Clearly the widening effect of the incision is not as accurate and precise as the effect of the toric IOL, but with experience the surgeon should and can anticipate his SIA for larger incisions, such as 3.0-3.5 mm.
Unfortunately, in this case, we no longer have the advantage of an MICS incision in terms of safety from the point of view of contamination, so that in this case one should be more careful.
Why is it better to refer to the Flattening Effect of the primary incision rather than the overall SIA vector (Surgical Induced Astigmatism) when calculating IOL power? The limitation of the SIA is that it depends on many factors and the surgeon must be aware of all these factors and adjust his or her SIA accordingly: size, location, architecture of the incision, furthermore corneal radius on a given meridian, corneal thickness, corneal elasticity, and also surgical technique, type of cataract (in particular the hardness of the nucleus) and dioptric value of the IOL to be implanted.
Of all these factors, the most important are the length of the incision (the longer the incision, the greater the induced astigmatism), the location of the incision (less astigmatism is induced on the temporal meridian than on the superior meridian) and the architecture of the incision - the shorter the tunnel to the centre, the greater the flattening effect on the meridian and the greater the induced astigmatism, and the longer the tunnel, the smaller the flattening effect on the meridian and the less significant the corneal changes.
Furthermore, when calculating a toric IOL, it must be taken into account that corneal alterations are produced not only on the incision meridian, but similarly on the opposite one at a distance of 90°: the incision creates a flattening effect on the meridian where it is made, and, at the same time, will cause an increase in the curvature of the other meridian, at a distance of 90° (effect 'coupling').
The SIA vector has two components: the flattening effect and the torsion; the former, the flattening effect, is the one that actually reduces astigmatism, whereas the torsion has no effect on the value of astigmatism (therefore no reduction on the incision meridian), but only changes the orientation of astigmatism (Borasio E, Mehta JS, Maurino V. Torque and flattening effects of clear corneal temporal and on-axis incisions for phacoemulsification. J Cataract Refract Surg. 2006 Dec;32(12):2030-8)
Dr Ozana Moraru
Oculus Eye Clinic Bucharest - Romania
E-mail: ozana@eye.ro
Please note that cookies are installed on this site by us and our selected partners to collect and process personal data from your devices (e.g. IP address, precise device tracking and geographical location),
Your consent is not required for the installation of technical and necessary cookies. For the others, however, you can freely give, refuse and revoke consent for the installation of all or some of the tracking systems and change your preferences by accessing the "Manage" section, which can be reached through the Cookie Policy or through this banner.I acceptI do not acceptRead more
You may revoke your consent at any time by using the Revoke Consent button.I want to delete cookies